ED – The European Journal of Vascular and Endovascular Surgery published over 120 recommendations. A few warrant discussion.
The definition of the abdominal aortic aneurysm (AAA) is based on the diameter of 3.0 cm or more. AAA is clinically mostly silent and abdominal assessment may not reveal it due to a poor sensitivity (<50%). The average growth rate is 1.3mm per year for 3 cm AAA, whilst 5 cm aneurysm grows almost three times faster. Risk factors are age, atherosclerosis, smoking, family history and hypertension whilst diabetes, on the other hand, is associated with lower rate of AAA.
scanned in ten-years intervals. Smoking cessation, blood pressure control, statin and antiplatelet therapy should be initiated for all patients with AAA of any size. Those reaching the threshold size for treatment (men 5.5 and women 5.0 cm) should be referred to a centre that performs more than 20 cases per year. Patients who have either poor functional capacity ( 4 METS) or those with unstable angina, decompensated heart failure, severe valvular diseases or arrhythmia should be referred for a cardiac workup.

Patients with no symptoms, those with stable coronary disease or those with asymptomatic carotid stenosis should not be routinely sent for coronary or carotid revascularisation. Preferred treatment option is endovascular aortic repair (EVAR) but young patients can be offered open repair.. In all patients, pulmonary function testing with spirometry prior to aortic surgery should be considered but chest x-ray is not
KEY MESSAGES
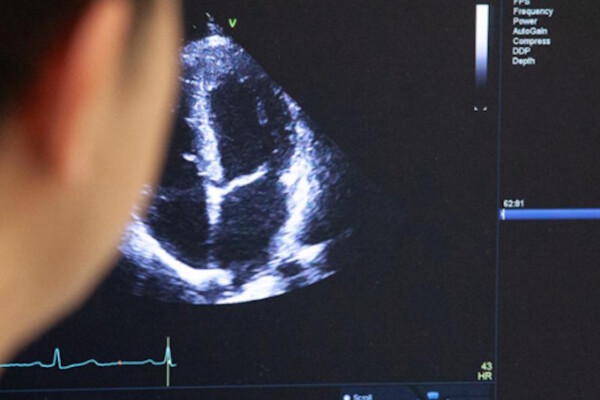
Ultrasound scan screening for men over 65 years.
Endovascular repair is the treatment of choice but young patients should be considered for open repair. Antiplatelet, antihypertensive and statin therapy is advised for all patients with any size of AAA.
Ultrasonography is recommended as the first line imaging for detection and also monitoring of AAA up to the size of 4.9 cm. Regardless of the aneurysm size, patients should be referred to a vascular Surgeon for evaluation except for cases with very short life expectancy. Population screening is still recommended for men Over 65 years of age but not for women, however, everyone over 50 years of age with a first line relative with AAA should be routinely recommended. Dual antiplatelet therapy after a coronary intervention is no contraindication for EVAR.